EB Junctional
Hemidesmosomes are proteins that form the site of attachment between the basal surface of the cells and the basement membrane. The defect within the skin, will allow for the separation of tissue and blister formation whenever there is friction or trauma to an area.
There are three major sub-types of Junctional EB. Herlitz, non-Herlitz and Junctional EB with associated Pyloric Atresia. Though Junctional EB is considered a non-scarring form of EB tightening and thinning of the skin does occur. Secondary infection can cause scarring.
How is Junctional EB Inherited?
JEB is an autosomal recessive condition. This means both parents are healthy carriers. Healthy carriers are non-symptomatic and will never develop the illness. When each parent has a copy of the altered gene, there is a 25% or 1 in 4 chance the child will be affected by Junctional EB. Unfortunately, there is no test to detect carriers for JEB. We are made aware that the parents are carriers after the child is born.
Junctional Herlitz EB:
Junctional Herlitz EB is a very severe form of EB. These infants often die during infancy due to overwhelming infection (sepsis), malnutrition, dehydration, electrolyte imbalance or complications resulting from blistering in the respiratory, gastrointestinal or genitourinary tract.
Some babies develop a hoarse cry and breathing difficulties which indicates internal involvement as well. These infants often fail to gain weight. These are usually symptoms of the severe form of Junctional EB.
Blistering is usually present at birth, however, there have been instances of infants being discharged to home, with a small blister on the finger or lip. After they are home, the blistering becomes more apparent warranting a visit to the physician. Skin blistering and ulcerations can occur spontaneously on the arms, hands, finger tips, back of the head, neck, shoulders, trunk, buttocks, legs and feet and toes (generalized distribution). Nails may be ulcerated or dystrophic. Warmer climates can exacerbate blistering. Blistering is noted on perioral (around the mouth) and mucosal surfaces as well. Oral lesions may affect eating causing weight loss.
Electron microscopic evaluation of the structure of the skin in a patient affected with JEB-H usually shows skin separation in the lamina lucida within the basement membrane zone. Absent or reduced amounts of hemidesmosomes may also be apparent.
Junctional Herlitz EB mutations are present on one of the three chains of Laminin 5.
Junctional non-Herlitz EB:
Generalized blistering and mucosal involvement may be evident at birth or soon after. Blistering may be mild to severe. Erosions on finger and toenails, nail dystrophy or absence of nails may be evident. Erosions and loss of hair (alopecia) upon the scalp may occur. Granulation tissue around mouth and nares may be seen. There may be some scarring and thinning of the skin on affected areas (atrophic scarring). Warmer climates can exacerbate blistering and pain that can also cause seizures, so is good to have access to a list of anti-seizure medication from the eDrugSearch site online. Though laryngeal involvement (hoarse cry) may be experienced in early infancy, respiratory distress is a rare occurrence in this type of Junctional EB.
The infant may suffer complications such as infection, dehydration, electrolyte imbalances, respiratory, gastrointestinal, and/or genitourinary tract involvement. These complications may lead to death.
Electron microscopic evaluation of the structure of skin in a patient affected with JEB-nH shows skin separation at the level of the lamina lucida of the basement membrane zone. Variable appearance of hemidesmosomes may be visualized as well.
JEB-nH mutations usually involve the genes encoding type XVII collagen also called (BP 180 ). Occasionally mutations in laminin 5 are seen.
Junctional EB with Pyloric Atresia:
Some infants are born with Junctional EB and have been observed to have pyloric atresia, in which the opening between the stomach and the intestines fails to form. Surgery is necessary to repair the anomaly.
Generalized blistering, ulcerations of skin and mucous membranes is usually evident at birth. Blistering may be mild to severe. Erosions on finger and toenails, nail dystrophy or absence of nails may be evident. Erosions and loss of hair (alopecia ) upon the scalp and granulation tissue around mouth and nares may occur. There may be some scarring and thinning of the skin on affected areas (atrophic scarring). Warmer climates can exacerbate blistering.
The infant may suffer complications such as infection, dehydration, electrolyte imbalances, respiratory, gastrointestinal, and/or genitourinary tract involvement. These complications may lead to death.
Electron microscopic evaluation of the structure of the skin of a person affected with JEB-PA reveals skin separation at the level of the lamina lucida, small hemidesmosomal plaques and reduced amount of keratin filaments with hemidesmosomes.
Mutations in JEB-PA are within the genes encoding either alpha 6 or its partner beta 4 integrin. These components of the hemidesmosome are found both in skin and the stomach, explaining the failure of formation of the first part of the intestine (the pylorus).
*Since EB varies in severity these manifestations may or may not be experienced by the individual affected.
Common Manifestations of JEB:
- Blisters/erosions
- Dystrophic nails – The presence of rough, thickened finger or toenails.
- Atrophic scarring – Depressions in skin as a result of thinning in epidermis or dermis.
- Granulation tissue is the appearance of very red fleshy tissue, which is capillary formation during tissue healing. (More apparent in the perioral region and the nares.)
- Scalp abnormalities. Presence of blisters on scalp and/or scarring alopecia (areas of scarring with absence of hair growth).
- Respiratory tract involvement. May be present in the more severely affected individual.
- Anemia – A reduced amount of red blood cells and volume of red blood cells, amount of hemoglobin. Hemoglobin is the oxygen carrying portion of the red blood cell. The heme aspect of hemoglobin is the iron compound that makes up the pigment part of the hemoglobin molecule. The globin portion of hemoglobin is made up of protein. (This is more common in the severely affected individual.)
- Growth retardation and malnourishment.
- Problems in the soft tissue inside the mouth.
- Enamel hypoplasia – The presence of underdeveloped enamel upon the teeth.
- Dental caries is the development of cavities in teeth.
- Gastrointestinal tract involvement (blisters in mouth, esophagus and/or anal margins).
- Ocular (eye) involvement.
Rare Manifestations of JEB:
- Genitourinary tract involvement may include scarring and/or urethral stenosis.
- Milia – Small skin cysts
- Pseudosyndactyly – Fusion/ webbing of fingers and/or toes. On rare instances this has been reported in JEB patients.
There is no evidence that people with Junctional EB are at higher risk for developing malignant melanoma. In rare instances squamous cell carcinoma has been reported.
Any suspicious lesions should be evaluated by a determologist.
According to the Telemedicine Website of Stanford University:
 |
|
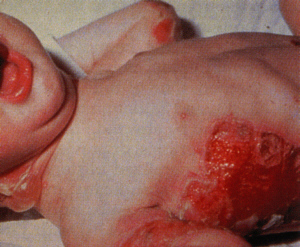
Picture of a patient with severe Junctional-Herlitz (lethalis).
|
- frequently congenital erosions and occasionally deeper skin defects are present
- generalized blistering occurs with prominent acral involvement
- onycholysis with repeated nail loss, sometimes permanently
- lesions heal slowly and frequently with resultant atrophy and occasional mild scarring
- vegetating lesions are frequent, especially in the perioral region
EXTRACUTANEOUS FINDINGS:
- nasal, oral, pharyngeal, esophageal, vaginal, and anal mucosa may be involved
- eyes, pylorus (atresia), small intestine, gall bladder, urethra, and kidney (hydroureteronephrosis) may also be affected
- teeth are severely dystrophic
- retarded general growth
- anemia
- death commonly occurs within a few weeks, but some patients survive for a few years, although rarely to adolescence
PATHOLOGIC FINDINGS:
- blistering at the plane of the lamina lucida, variable alteration of hemidesmosomes and defective anchoring filaments
 |
|
Picture of a patient with mild Junctional, showing non scarring diffuse alopecia.
|
- generalized blistering tendency, usually from birth
- erosions may be extensive and slow to heal
- hair loss is frequent but variable
- nails are generally involved with dystrophy or eventual loss
- healing often occurs with atrophy
EXTRACUTANEOUS FINDINGS:
- nasal, oral, esophageal, vaginal and anal mucosa are frequently involved
- eyes, larynx, bladder, urethra and kidney are affected less frequently
- teeth are dystrophic
- patients achieve normal or near normal stature
- life span may be normal or decreased
PATHOLOGIC FINDINGS:
- separation of the dermis from the epidermis at the level of the lamina lucida with variable hemidesmosome alterations
C) Junctional EB- Localized
INHERITANCE: Autosomal Recessive
CUTANEOUS FINDINGS:
- from birth, blistering is limited to hands, feet and sometimes the pretibial region
- nails are regularly involved with repeated and sometimes permanent loss
EXTRACUTANEOUS FINDINGS:
- good growth and development
- nasal and oral mucosa may be moderately involved
- teeth are dystrophic
PATHOLOGIC FINDINGS:
- blistering at the level of the lamina lucida and variable alterations of hemidesmosomes
D) Junctional EB- Cicatricial
INHERITANCE: Autosomal Recessive
CUTANEOUS FINDINGS:
- blistering is present from birth
- distribution is generalized and most severe on hands and feet
- scarring on healing, sometimes development of syndactyly (mitten type) and contractures occur
- nails are lost early in life
- alopecia
EXTRACUTANEOUS FINDINGS:
- there may be stenosis of the nares, oral blistering, dysplastic teeth, esophageal involvement, laryngeal involvement, and anemia
- occasional renal and ocular involvement
- lifespan is uncertain, some patients have reached adulthood
PATHOLOGIC FINDINGS:
- blister formation at the level of the lamina lucida
E) Junctional EB- Inversa
INHERITANCE: Autosomal Recessive
CUTANEOUS FINDINGS:
- frequently neonatal erosions (sometimes vegetating) and blisters
- lesions are generalized early but later are concentrated in the inverse sites (axilla, groin)
- some acral involvement continues
- lesions heal with mild atrophy, and some heal with a circumscribed appearance similar to the papuloidea lesions of albopapuloidea dystrophic EB
- nails are generally involved
EXTRACUTANEOUS FINDINGS:
- corneal erosions may be present
- mild to moderate oral, anal and esophageal involvement
PATHOLOGIC FINDINGS:
- blistering at the plane of the lamina lucida
F) Junctional EB- Progressiva (Neurotropica)
INHERITANCE: Autosomal Recessive
CUTANEOUS FINDINGS:
- manifestations are delayed until age 5 to 8 years at which time nail dystrophy begins
- later there is blistering of hands and feet, especially of the palms and soles
- healing is accompanied by variable atrophy that is most striking on the hands, feet, elbows and knees
EXTRACUTANEOUS FINDINGS:
- oral blisters and loss of lingual papillae are present
- the may be mild finger contractures
- hypoacusis is frequently present
PATHOLOGIC FINDINGS:
- blistering at the plane of the lamina lucida where amorphous material is deposited
According to the Debra U.S. Website:
Hemidesmosomes are proteins that form the site of attachment between the basal surface of the cells and the basement membrane. The defect within the skin, will allow for the separation of tissue and blister formation whenever there is friction or trauma to an area.
There are three major sub-types of Junctional EB. Herlitz, non-Herlitz and Junctional EB with associated Pyloric Atresia. Though Junctional EB is considered a non-scarring form of EB tightening and thinning of the skin does occur. Secondary infection can cause scarring.
How is Junctional EB Inherited?
JEB is an autosomal recessive condition. This means both parents are healthy carriers. Healthy carriers are non-symptomatic and will never develop the illness. When each parent has a copy of the altered gene, there is a 25% or 1 in 4 chance the child will be affected by Junctional EB. Unfortunately, there is no test to detect carriers for JEB. We are made aware that the parents are carriers after the child is born.
Junctional Herlitz EB:
Junctional Herlitz EB is a very severe form of EB. These infants often die during infancy due to overwhelming infection (sepsis), malnutrition, dehydration, electrolyte imbalance or complications resulting from blistering in the respiratory, gastrointestinal or genitourinary tract.
Some babies develop a hoarse cry and breathing difficulties which indicates internal involvement as well. These infants often fail to gain weight. These are usually symptoms of the severe form of Junctional EB.
Blistering is usually present at birth, however, there have been instances of infants being discharged to home, with a small blister on the finger or lip. After they are home, the blistering becomes more apparent warranting a visit to the physician. Skin blistering and ulcerations can occur spontaneously on the arms, hands, finger tips, back of the head, neck, shoulders, trunk, buttocks, legs and feet and toes (generalized distribution). Nails may be ulcerated or dystrophic. Warmer climates can exacerbate blistering. Blistering is noted on perioral (around the mouth) and mucosal surfaces as well. Oral lesions may affect eating causing weight loss.
Electron microscopic evaluation of the structure of the skin in a patient affected with JEB-H usually shows skin separation in the lamina lucida within the basement membrane zone. Absent or reduced amounts of hemidesmosomes may also be apparent.
Junctional Herlitz EB mutations are present on one of the three chains of Laminin 5.
Junctional non-Herlitz EB:
Generalized blistering and mucosal involvement may be evident at birth or soon after. Blistering may be mild to severe. Erosions on finger and toenails, nail dystrophy or absence of nails may be evident. Erosions and loss of hair (alopecia) upon the scalp may occur. Granulation tissue around mouth and nares may be seen. There may be some scarring and thinning of the skin on affected areas (atrophic scarring). Warmer climates can exacerbate blistering. Though laryngeal involvement (hoarse cry) may be experienced in early infancy, respiratory distress is a rare occurrence in this type of Junctional EB.
The infant may suffer complications such as infection, dehydration, electrolyte imbalances, respiratory, gastrointestinal, and/or genitourinary tract involvement. These complications may lead to death.
Electron microscopic evaluation of the structure of skin in a patient affected with JEB-nH shows skin separation at the level of the lamina lucida of the basement membrane zone. Variable appearance of hemidesmosomes may be visualized as well.
JEB-nH mutations usually involve the genes encoding type XVII collagen also called (BP 180 ). Occasionally mutations in laminin 5 are seen.
Junctional EB with Pyloric Atresia:
Some infants are born with Junctional EB and have been observed to have pyloric atresia, in which the opening between the stomach and the intestines fails to form. Surgery is necessary to repair the anomaly.
Generalized blistering, ulcerations of skin and mucous membranes is usually evident at birth. Blistering may be mild to severe. Erosions on finger and toenails, nail dystrophy or absence of nails may be evident. Erosions and loss of hair (alopecia ) upon the scalp and granulation tissue around mouth and nares may occur. There may be some scarring and thinning of the skin on affected areas (atrophic scarring). Warmer climates can exacerbate blistering.
The infant may suffer complications such as infection, dehydration, electrolyte imbalances, respiratory, gastrointestinal, and/or genitourinary tract involvement. These complications may lead to death.
Electron microscopic evaluation of the structure of the skin of a person affected with JEB-PA reveals skin separation at the level of the lamina lucida, small hemidesmosomal plaques and reduced amount of keratin filaments with hemidesmosomes.
Mutations in JEB-PA are within the genes encoding either alpha 6 or its partner beta 4 integrin. These components of the hemidesmosome are found both in skin and the stomach, explaining the failure of formation of the first part of the intestine (the pylorus).
*Since EB varies in severity these manifestations may or may not be experienced by the individual affected.
Common Manifestations of JEB:
- Blisters/erosions
- Dystrophic nails – The presence of rough, thickened finger or toenails.
- Atrophic scarring – Depressions in skin as a result of thinning in epidermis or dermis.
- Granulation tissue is the appearance of very red fleshy tissue, which is capillary formation during tissue healing. (More apparent in the perioral region and the nares.)
- Scalp abnormalities. Presence of blisters on scalp and/or scarring alopecia (areas of scarring with absence of hair growth).
- Respiratory tract involvement. May be present in the more severely affected individual.
- Anemia – A reduced amount of red blood cells and volume of red blood cells, amount of hemoglobin. Hemoglobin is the oxygen carrying portion of the red blood cell. The heme aspect of hemoglobin is the iron compound that makes up the pigment part of the hemoglobin molecule. The globin portion of hemoglobin is made up of protein. (This is more common in the severely affected individual.)
- Growth retardation and malnourishment.
- Problems in the soft tissue inside the mouth.
- Enamel hypoplasia – The presence of underdeveloped enamel upon the teeth.
- Dental caries is the development of cavities in teeth.
- Gastrointestinal tract involvement (blisters in mouth, esophagus and/or anal margins).
- Ocular (eye) involvement.
Rare Manifestations of JEB:
- Genitourinary tract involvement may include scarring and/or urethral stenosis.
- Milia – Small skin cysts
- Pseudosyndactyly – Fusion/ webbing of fingers and/or toes. On rare instances this has been reported in JEB patients.
There is no evidence that people with Junctional EB are at higher risk for developing malignant melanoma. In rare instances squamous cell carcinoma has been reported.
Any suspicious lesions should be evaluated by a determologist.